
Company Spotlight: Somnee
A 15-minute Somnee session before bed is all you need to improve your whole night.

In one of my most recent posts, I covered Prophetic’s mission of inducing lucid dreams using focused ultrasound. That sounds great, but it can be difficult to fall asleep most of the time—it’s not like you can pass out whenever you like.
That’s where Somnee comes in. This Berkeley company makes the Smart Headband to help you fall asleep faster and sleep more efficiently. It includes an electroencephalography (EEG) sensor to record your brain state at bedtime and an electrode for transcranial electrical stimulation (tES), which will stimulate the brain for 15 minutes to induce a more restful state. Because the precise way your brain is stimulated depends on how the headband interprets its signals, this makes it one of the few closed-loop BCIs on the market.

As outlined in their research paper, the Berkeley researchers combine two technologies in a novel way. tES (more specifically, transcranial alternating current stimulation or tACS) is a non-invasive way of stimulating the brain with no harmful side effects. Previous studies have found that stimulating the frontal cortex at 5 Hz can make patients drowsy. EEG, which records a jumble of neuronal activity, can provide biomarkers for sleep quality. Everyone has slightly different baseline activity levels recorded by EEG, so they tried both a fixed stimulatory pattern and one tailored for each patient based on their EEG.
EEG signals are typically transformed from time-domain into frequency domain using a Fourier Transform. So, instead of looking at the signals over time, you see how strong the signal is at 1 Hz, 5 Hz, 10 Hz, 60 Hz, etc. Neuroscientists usually separate the frequencies into bands that act as biomarkers, like the alpha band (8 - 13 Hz) and theta band (4 - 8 Hz).
Here is an example of a frequency-domain graph with the bands identified, from this paper.
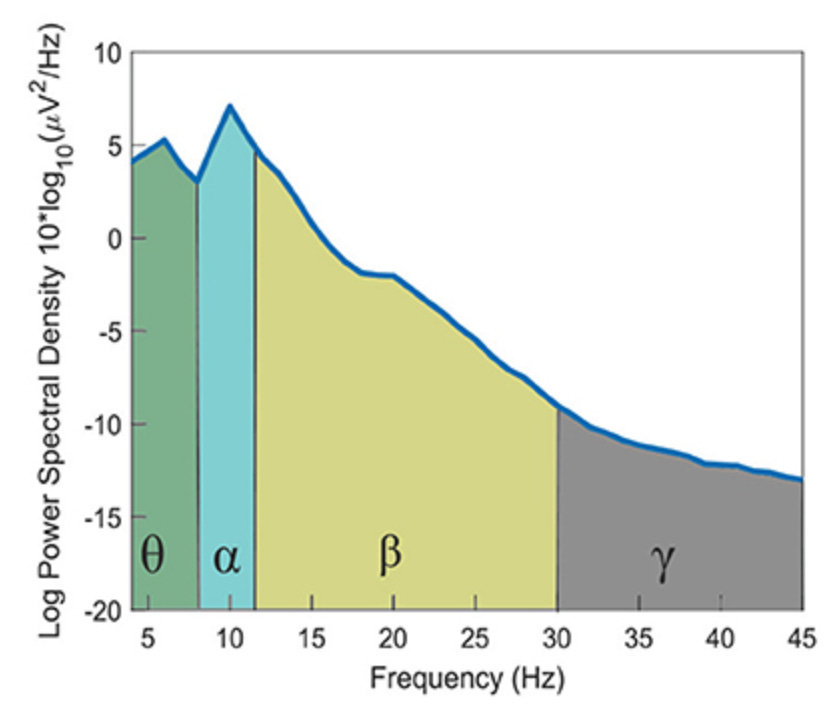
For the fixed tACS stimulation, the researchers applied two in-phase 10 Hz and 5 Hz sinusoidal waves to target the alpha and theta bands respectively. They chose them because alpha band activity (8–13 Hz) is linked to stage I sleep and theta band activity (4–8 Hz) is linked to the transition to stage II sleep, according to another study. The amplitude of the waves was 0.6 mA peak-to-peak.
For the personalized tACS stimulation, the researchers took EEG samples of patients in a relaxed, closed-eyed state (similar to someone laying down to sleep), and they identified the peak closest to 5 Hz within 4-6 Hz and the peak closest to 10 Hz within 9-11 Hz. They then applied similar sinusoidal waves as the fixed stimulation, just with the slightly-changed frequencies for the two sine waves. They started in phase, but didn’t remain that way unless the 5 Hz-adjacent wave was half the frequency of the 10 Hz-adjacent one.
They also tested a sham session without stimulation and measured sleep quality with a Fitbit. For either one, you don’t actually have to wear the headband to sleep. You can just wear it for the 15-minute stimulation and take it off to sleep. If it works, you would expect the personalized stimulation to outperform the fixed one, which would outperform the sham. If it doesn’t work, would I be writing this blog post?
Let’s check the results.
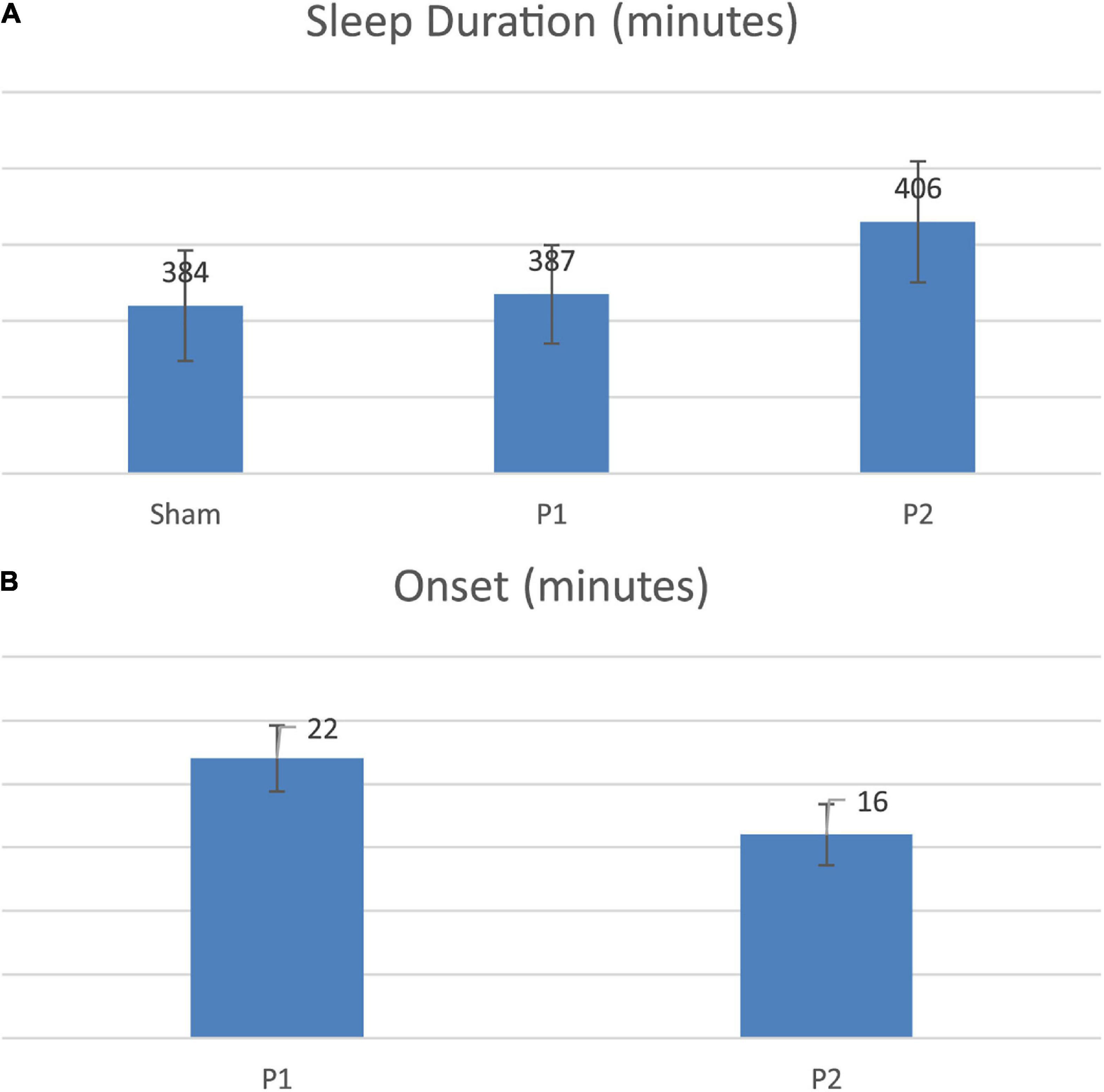
P1 refers to fixed stimulation, and P2 refers to tailored stimulation. I wish they would change their graphs from the Excel default, but other than that, they show that people who use the personalized stimulation fall asleep faster (B) and sleep longer (A) than people who even use the fixed stimulation. Why don’t they have the sleep onset bar for the sham? My guess it that the number is not comparable, since those people don’t stay up for 15 minutes receiving the stimulation.
I’m surprised that the P1 patients slept for essentially as long as the sham ones. The only difference between P1 and P2 is at most a 1 Hz change in the frequency of both of the sinusoids. Maybe the fact that the fixed stimulation waves are harmonics of each other masks their effect somehow, so if they applied 4.9 Hz and 10.1 Hz instead of 5 Hz and 10 Hz it would remove that problem. That’s just pure speculation, though. This paper points to other papers that show open-loop (non-personalized) stimulation can improve sleep, but this paper seems to refute that idea. The other papers use either transcranial magnetic stimulation (TMS), auditory stimulation, or transcranial direct current stimulation (tDCS) during sleep, while this paper uses alternating current tACS before sleep. Maybe there’s something about tACS or applying it before sleep that doesn’t improve sleep quality, or maybe those papers are measuring sleep quality using a metric other than duration.
The authors actually wonder the same thing in their conclusion, and they have the same idea about the harmonic nature of their fixed stimulation. They should just hire me at this point. They also point to their small sample size.
Either way, let’s not let this mystery and the default Excel graphs take away from the result: that there is a way to apply a current to your brain for 15 minutes that helps you sleep longer. Imagine if one day, we can have implanted electrodes that can stimulate the right neurons to trigger your brain to sleep at the push of a button. Or even ones that can inhibit it. Is there a way to apply tACS in a way that makes you less drowsy? You can use that to lock in at critical moments, like driving home after a long night or staying awake for an 8 AM meeting. I can’t wait for the future.